In the world of high-performance sports and competitive bodybuilding, the pursuit of peak physical condition often involves complex physiological trade-offs. While much focus is placed on muscle hypertrophy and recovery, the cardiovascular system frequently bears a heavy, invisible burden. For athletes utilizing performance-enhancing substances, the challenge is not just "high blood pressure" in the traditional sense, but a systemic shift in blood chemistry known as secondary polycythemia.
The Mechanism: Blood Pressure vs. Blood Density
In a healthy athlete, blood pressure is regulated by the heart's output and the resistance of the blood vessels. However, certain training protocols and pharmacological aids can disrupt this balance through two primary pathways:
-
Water and Sodium Retention: Some substances mimic aldosterone, a hormone that causes the body to hold onto salt and water. This increases the total volume of blood in the system, forcing the heart to pump harder against higher pressure.
-
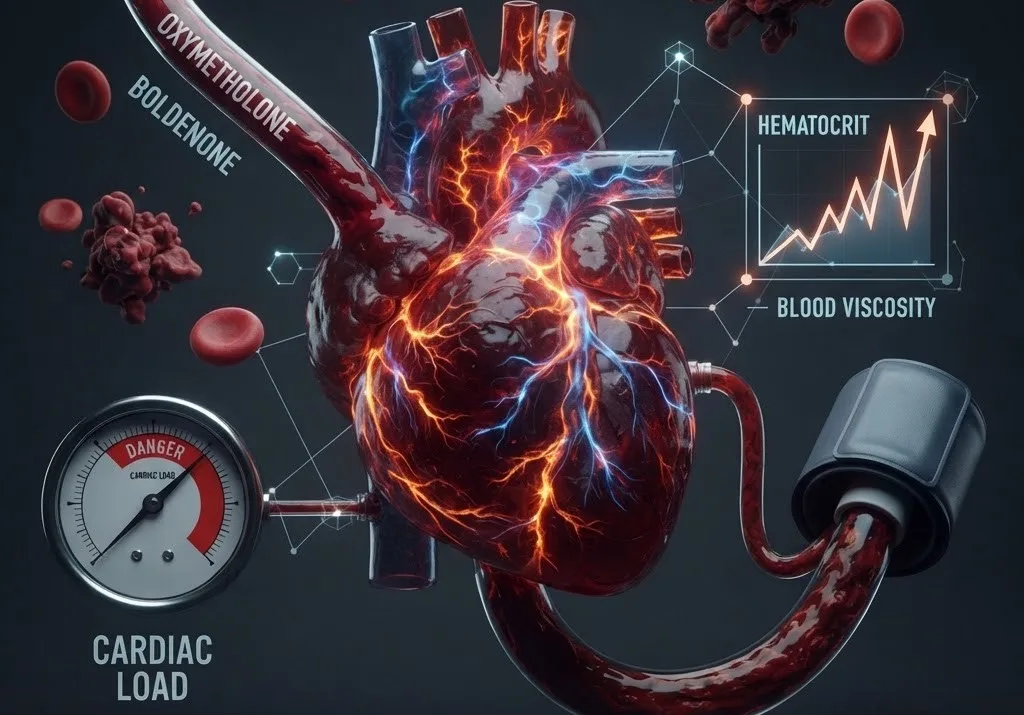
Increased Erythropoiesis (RBC Production): Many performance aids stimulate the production of Red Blood Cells (RBCs). While this can improve oxygen delivery in the short term, it eventually leads to Hyperviscosity—where the blood becomes "thick."
When the concentration of red blood cells (hematocrit) rises significantly, the blood behaves more like syrup than water. This thick blood requires more force to move through the capillaries, naturally driving up blood pressure.
The Nitric Oxide Deficit
One of the most critical side effects of high hematocrit levels is the suppression of Nitric Oxide (NO). Nitric Oxide is a gas produced by the endothelium (the inner lining of blood vessels) that signals the vessels to relax and dilate (vasodilation).
As blood density increases, the shear stress on the vessel walls changes, often impairing the natural release of NO. Without adequate NO, the blood vessels remain constricted even when the athlete is at rest, creating a state of chronic hypertension that is resistant to standard lifestyle interventions like "cardio" or "clean eating."
Choosing the Right Management Strategy
Athletes often face a dilemma: should they use clinical medications or address the underlying blood thickness?
1. Pharmacological Intervention
Medical combinations like Calcium Channel Blockers (e.g., Amlodipine) and Angiotensin II Receptor Blockers (ARBs) (e.g., Valsartan) are standard for clinical hypertension.
-
Amlodipine works by relaxing the smooth muscles of the blood vessels.
-
Valsartan blocks the hormone that causes vessels to tighten.
While effective, some athletes argue that these medications are merely "masking" the pressure without fixing the density of the blood. Furthermore, for competitive athletes, some antihypertensives (like diuretics or beta-blockers) are prohibited by governing bodies because they can mask other substances or reduce athletic performance.
2. Physiological Management: Phlebotomy
For the athlete dealing specifically with steroid-induced polycythemia, many practitioners suggest therapeutic phlebotomy (bloodletting). By physically removing a unit of blood, the body is forced to replace the volume with plasma (water), effectively "thinning" the blood and lowering the hematocrit. This often results in an immediate drop in blood pressure because the heart no longer has to push such a dense fluid through the system.
Summary Table: Blood Pressure Management in Athletes
| Factor | Mechanism | Athletic Impact |
| High Hematocrit | Increases blood viscosity (thickness). | Increases heart strain; raises stroke risk. |
| Nitric Oxide | Promotes vasodilation (widening). | Improves blood flow and reduces pressure. |
| ARBs/CCBs | Relaxes blood vessel walls. | Effective but doesn't fix blood "thickness." |
| Phlebotomy | Reduces red blood cell count. | Directly addresses blood density. |
Conclusion
For the modern athlete, blood pressure is not a single-digit problem to be solved with a single pill. It requires a nuanced understanding of how blood density, hormonal balance, and vascular health intersect. Regular blood work—specifically monitoring Hemoglobin and Hematocrit—is the only way to distinguish between "simple" hypertension and the more complex challenges of thick blood.